Evidence-based practice in Marriage & Family Therapy Curricula
(Marlowe, Cannata, Bertram, Kerns, Choi)
- This was the second in a series of Consortium studies on workforce development at the interface of academic and behavioral health care programs. It was approved by the University of Washington’s IRB. Principle investigator is Sue Kerns PhD. Participating researchers include Rosalyn Bertram PhD. LMFT; Elisabeth Cannata PhD; Dana Marlowe PhD; Soo-Whan Choi MA Doctoral candidate, and Sophie Wolfe (MSW candidate)
- This study replicates the Consortium’s exploration of evidence-based practice in North American MSW curricula study (Bertram, Charnin, Kerns, & Long, 2014; 2015).The full report of this study and the summary article published in the Journal of Research on Social Work Practice are available for review from the RESOURCES tab on this website.
ABSTRACT
This study is the second in a series that examines the extent to which master’s level professional degree programs teach evidence-based practices (EBPs). The first examined North American MSW curricula (Bertram, Charnin, Kerns, & Long, 2015). This second study focuses upon master’s level Marriage and Family Therapy (MFT) programs. Participants included program chairs or directors from 27 COAMFTE-accredited programs (30% response rate). Surveys were completed on-line or via telephone interview. The survey assessed program demographics, EBPs taught, depth of instruction, and whether underlying skills associated with EBP were included. The majority of programs (n = 23; 85%) taught EBP though there was a range in the number taught and depth of instruction. Qualitative responses indicated benefits and challenges for integrating EBP into course curriculum. Implications of findings are discussed.
Evidence-based practice in Marriage & Family Therapy Curricula
This study is the second in a series that examines the extent to which master’s level professional degree programs teach evidence-based practices (EBPs). The first examined North American MSW curricula (Bertram, Charnin, Kerns, & Long, 2015). This second study focuses upon master’s level Marriage and Family Therapy (MFT) programs. These studies emerged from the Child and Family Evidence Based Practice Consortium, an international and interdisciplinary group that supports the dissemination and implementation of behavioral health care practices demonstrating strong empirical support.
In a workforce readiness survey conducted by a Canadian Consortium participant, 589 North American behavioral health care administrators and clinical supervisors indicated that new master’s level practitioners were not well-prepared to deliver EBPs. Respondents reported that clinicians frequently learn about evidence-based practice after they are hired. In addition to lacking the technical skills to deliver specific interventions, they often lack skills to search for and critically appraise literature to support a scientific approach to practice, and these skills are developed through agency training and coaching (Barwick, 2011). These findings inspired a group of Consortium researchers to initiate a series of studies that examine the extent to which master’s level professional degree programs teach specific evidence-based practices and the underlying skills needed to identify and apply evidence-based practices.
METHOD
Design
The study design is a cross-sectional, point-in-time, survey. IRB exempted review approval was obtained from the University of Washington.
Recruitment of participants
Participating programs were identified and recruited using the COAMFTE list of MFT programs and directors (coamfte.org). Outreach began in 2015 via two email invitations sent to the MFT program directors’ listserv by the director of an accredited program. This approach did not yield a sufficient sample size. To ensure geographic representation and a range of different program sizes, in 2016 we applied targeted recruitment strategies that included personalized e-mail invitations to each program chair or director followed by a phone call invitation. Participants were told that responses would be confidential and would not identify their university or program. This adjustment to sampling yielded responses from 27 of the 89 accredited master’s degree programs in Marriage and Family Therapy (30% response rate).
Procedure
In most cases, the directors completed the survey. In a few instances, the director appointed another faculty member with depth of program knowledge to respond. Respondents could complete the survey via a web-based link or via telephone interview. Prior to completing the survey, respondents were provided a tool designed to support gathering further information about each EBP from other faculty. Telephone interviews were scheduled to last approximately 30 minutes and were conducted by several authors (Kerns, Bertram, Cannata, & Marlowe)
Survey Instrument
The same survey as in the study of MSW curricula was utilized, adapting language to reflect queries about MFT programs instead of MSW programs. The same criteria for defining an EBP used in the MSW curricula study (Bertram, Charnin, et al., 2015), in Barwick’s investigation (2011) and in previous research (Chambless & Ollendick, 2001; Silverman & Hinshaw, 2008) were also applied and included the following: (a) a clearly defined target population; (b) written elements, activities, and phases of service delivery; and (c) research supporting effectiveness with that population established through random-assignment control group (RCT) studies.
The adapted survey sought information on MFT program demographics and curricula characteristics. These included (a) geographic region, (b) total number of full and part-time students, (c) whether or not EBPs that meet study criteria are taught, (d) names of EBPs taught, (e) total number of faculty by position, and (f) by position, the number teaching EBPs. Faculty positions were differentiated by traditional tenure track titles (i.e., professor, associate professor, and assistant professor) and non-tenure track instructor and adjunct faculty positions.
As with the MSW curricula study, this survey used the National Implementation Research Network’s (NIRN) intervention component framework (Bertram, Blase, & Fixsen, 2015; Fixsen, Blase, Naoom, & Wallace, 2009) to query respondents on the depth and extent to which each identified EBP was taught. This framework includes: (a) clearly identified elements, participants, activities and phases; (b) the theory base(s) supporting them; (c) research supporting the efficacy of this practice with specific client populations; and (d) the practice model’s theory of change. Thus, for each identified EBP, respondents were asked: Is the research supporting application of this EBP with a client population taught? Are the elements, activities, participants and phases of delivery taught for this EBP? Are the theory base(s) supporting this taught? And, is the theory of change taught? Respondents could reply (a) yes, (b) no, or (c) don’t know to each of these five questions. Further, for each EBP, we inquired if students had opportunities to apply this EBP in course assignments or in field learning sites.
For comparison with Barwick’s study (2011), three questions asked respondents to rate how well their MFT program developed student skill sets that support evidence-based practice. This included search, critical appraisal, and scientific approach skills. Search skills were defined as knowledge of secondary sources of reliable information about evidence-based programs or promising practices. Critical appraisal skills were defined as the ability to accurately appraise research findings for validity, impact, and applicability and to draw on clinical expertise to integrate this knowledge with client information. A scientific approach to knowledge building was defined as the ability to formulate a clinical problem, develop or utilize the appropriate intervention strategy, and evaluate service delivery for outcomes. These questions were answered via a 4-point scale ranged from 0 (not at all addressed), 1 (minimally/briefly addressed), 2 (somewhat addressed), and 3 (thoroughly/extensively addressed). Finally, we asked respondents to present their perspectives regarding barriers and challenges to teaching evidence based practices and to discuss their perspectives of the positive or negative implications of teaching evidence-based practices in master degree MFT programs.
Analysis
Quantitative data analysis used SPSS (version 23). Due to sample size, we could not conduct inferential statistics. Descriptive statistical analysis included measures of central tendency and frequency. Qualitative data analysis applied a grounded theory approach to code responses and identify themes. Open-ended responses to survey questions about barriers, and the positive and negative implications of the current emphasis on the use of EBPs as well as to teaching evidence-based practice were independently reviewed by two study team members (Cannata & Marlowe). Each identified recurring themes that were then compared, clarified, and theme-coded. All responses were again independently reviewed and theme-coded. This final independent coding was compared and discussed to resolve discrepancies resulting in theme frequency counts.
RESULTS
Program demographics
Of the twenty-seven accredited master degree programs in Marriage and Family Therapy that completed the survey, eight (30%) were from Northeastern states, seven (26%) from Midwestern states, seven (26%) from Western states, and five (18.5%) from Southern states.
Program size varied, with from 8 to 68 full and part-time students pursuing a master degree in the 2017 academic year (M = 23.64, SD = 15.06). Faculty size was usually small, but ranged from two to as many as eighteen faculty (M = 9.85, SD = 4.56). Five (18.5%) of the universities surveyed also offered the DMFT or Ph.D. degrees in marriage and family therapy.
Presence of EBPs in MFT programs
Thirty-seven practice models were identified by respondents as an evidence-based practice that met study criteria. Nominated practices were coded (i.e., met versus not met) against the study’s definitional criteria by five raters from the study team (Bertram, Cannata, Choi, Kerns, & Marlowe). Determination of met or not met was made by consulting secondary databases such as the National Registry of Evidence Based Programs and Practices (NREPP; www.nrepp.samhsa.gov), Blueprints for Healthy Youth Development (http://www.blueprintsprograms.com), and the California Evidence Based Clearinghouse (CEBC; http://www.cebc4cw.org). We also found and reviewed original research when a program was either (a) not listed in the secondary databases, or (b) there were conflicting ratings across the different databases. Discrepancies between raters were resolved through in-depth literature searches and reviews, and by enlisting an additional rater with EBP expertise from outside the study team to review the 37 nominated practice models. This procedure yielded an interrater reliability rating of 98% with 26 of the 37 practice models meeting study criteria.
Programs that did not teach specific EBPs. Four programs indicated that they do not teach any EBPs. Two were in the Midwest, one in the West, and one in the South. These programs reported enrollments of 24 to 40 students, thus were in the mid to upper range of MFT program size.
Programs providing minimal exposure to specific EBPs. In addition to the four programs that did not teach specific EBPs, some programs provided only minimal exposure. Two noted that students may receive training in an EBP when they are in their placement setting but did not have formal inclusion within class syllabi. One indicated there was opportunity for exposure to specific EBPs through an elective course, but this was not a core part of its curricula. Two programs indicated they provide basic information about EBPs in research courses.
Programs teaching specific EBPs. The majority of programs teach EBPs (n = 23; 85%). Examination of what faculty positions teach course content related to EBP revealed that tenure track faculty are more likely to teach EBPs than other faculty. Specifically, 85% of full professors, 61% of associate professors, and 70% of assistant professors taught EBP, compared with 46% of instructors and 45% of adjunct faculty.
Student enrollment, number of EBPs, and faculty size. Most programs that taught specific evidence based practices reported annual enrollments of less than 24 students. The size of the faculty in these programs was also small, ranging from two to six. There was a range of specific EBPs taught (see Table 1). Where EBPs were taught, the number ranged from 1-10 (10 being the most allotted by the survey). Emotion Focused Therapy and two closely related variants were by far the most common, with two thirds of programs indicating that they teach this treatment model. Functional family therapy (FFT), Mutisystemic therapy (MST), and Cognitive Behavioral Therapy (CBT) were the next most commonly taught interventions. The remaining EBPs were taught by a quarter or less of MFT programs. Not listed in the table are EBPs that were only taught in one MFT program. These included: Integrative Cognitive Behavior Therapy, Solution Focused Brief Therapy, Brief Strategic Family Therapy, Attachment Based Therapy, Child Centered Play Therapy, Collaborative Problem Solving, FAST Families and Schools Together, Helping the Non-Compliant Child, The Incredible Years, Integrative Couples Therapy, Interactive Behavioral Couples Therapy, Parent Management Therapy- Oregon, PREP (relationship education), and Strengthening Families (Age 10-14).

Regional differences
Although the number of responding programs from southern states was smaller than other geographic regions, these programs taught a greater number and variety of specific EBPs. Emotion Focused Therapies and FFT were taught in all geographic regions, while MST was only taught in the Northeastern and Western states. Table 2 presents EBPs taught in each region, student enrollment, number of faculty and the number of faculty teaching those EBPs.

Northeast. The eight responding programs from northeastern states reported teaching Functional Family Therapy (FFT; n = 5), Multisystemic Therapy (MST; n = 5), Multidimensional Family Therapy (n = 5), Cognitive Behavioral Therapy (CBT; n = 4), Emotion Focused or Emotionally Focused Couples Therapy (n = 4).
Midwest. The eight responding programs from midwestern states reported teaching CBT or Trauma Focused Cognitive Behavioral Therapy (TF-CBT; n = 4), Emotion Focused Therapy (n = 3), FFT (n = 2), and Structural Family Therapy (n = 2).
West. The seven responding programs from western states reported teaching Emotion Focused Therapy (n = 6), FFT (n = 3) and MST (n = 3).
South. The five responding programs from southern states reported teaching CBT, TF-CBT, and Integrative Cognitive Behavioral Therapy (n = 5), Emotion Focused or Emotion Focused Marriage and Family Therapy (n = 5), FFT (n = 3), Gottman Therapy (n = 3), and Structural Family Therapy (n = 3).
Depth and extent of instruction
Most programs (n = 22) reported teaching all intervention components of an EBP for at least one EBP. This included not only the research supporting its effectiveness with specific client populations and the elements, activities, participants and phases of service delivery, but also the theory base(s) supporting the model(s) and the practice model’s theory of change. In addition to this thorough presentation of the identified EBP, most programs (n = 21) reported that students were provided the opportunity in field settings or in course assignments to apply the practice model in at least one EBP.
When EBPs were not thoroughly presented, the lack of thoroughness was not consistent. For example, in a program that reported teaching Emotion-Focused Therapy; Structural Family Therapy; Strategic Family Therapy; and Solution-Focused Therapy, all NIRN intervention components were presented to students learning Emotion-Focused Therapy. Students learning Structural Family Therapy were not taught its elements, activities, participants and phases, but were presented with its theory base, theory of change, and research supporting its effectiveness with specific client populations. In contrast, the related theory bases for Strategic Family Therapy and Solution Focused Therapy were not taught but all other NIRN intervention components were. Another program taught Emotion-Focused Therapy, Attachment Based Therapy, and CBT, but only the research supporting effectiveness with specific client populations and theory base for each were presented.
One program taught MST, MDFT, and Emotion Focused Therapy. MDFT and Emotion-Focused Therapy were presented thoroughly (all NIRN intervention components). MST instruction included all NIRN intervention components except its elements, activities, participants and phases of service delivery. This was notable since MST elements and activities are so clearly and specifically described (Henggeler, Schoenwald, Borduin, Rowland, & Cunningham, 2009). Also notable, was the variability in presentation of different models in one program that taught TFCBT, MST, PCIT, FFT, and Emotion Focused Therapy. There, all NIRN intervention components were presented for TFCBT, MST and Emotion Focused Therapy. Presentation of PCIT included all intervention components except research supporting its effectiveness with specific populations. Presentation of FFT included all intervention components except its theory of change and research supporting its effectiveness with specific populations. This stood out since these interventions components are readily available for presentation to students.
Comparison with Barwick (2011) study
For comparison with Barwick’s study (2011), respondents rated how well their MFT program developed student skill sets that support evidence-based practice.
Critical appraisal skills. This was defined as the ability to accurately appraise research findings for validity, impact, and applicability to client information. Barwick’s 2011 study indicates that over half (56%) of the responding behavioral health program administrators and supervisors perceived this as an essential skill to effectively deliver EBPs, while 55% indicated that practitioners with master degrees did not possess this ability when they entered the workforce.
Two thirds of the MFT programs (n = 18, 66%) indicated they thoroughly or extensively addressed critical appraisal skills. These skills were somewhat addressed in eight programs (30%), with only one program indicating it minimally or briefly addressed the development of these skills.
Search techniques. This was defined as the ability to find secondary sources of reliable information pertaining to evidence-based programs or practices. In Barwick’s (2011) study, this skill was identified as important for EBP practice by 43% of the responding behavioral health program administrators and supervisors, while 54% of the respondents noted that newly hired masters level practitioners did not possess this skill upon hire.
Of the 27 responding MFT programs, ten (37%), reported they thoroughly or extensively addressed student development of search techniques. Eight programs (29%) reported somewhat addressing development of these skills. Seven (26%) reported that their program minimally or briefly addressed development of these skills, and two programs (7%) indicated they did not attempt to develop these skills.
Scientific approach to knowledge. This was defined as the ability to formulate a clinical problem, develop or apply the appropriate practice, and evaluate service delivery for outcomes.
In Barwick’s study (2011), the majority (69%) of the responding behavioral health program administrators and supervisors identified this skill as necessary to effectively deliver an EBP. However, 64% of those respondents reported that master’s level practitioners did not possess this skill set and had to develop it upon hire.
In our study, seventeen MFT programs (63%) indicated they thoroughly or extensively taught students a scientific approach to knowledge. Nine programs (33%) indicated they somewhat addressed this, while one program reported that this skill was only minimally or briefly addressed within its curriculum.
Qualitative responses
Finally, we asked respondents to present their perspectives of barriers and challenges to teaching evidence based practices, and to identify positive or negative implications of an emphasis on use of EBPs in the field of marriage and family therapy. Twenty (74.1%) respondents identified advantages for students or for the field, and 25 (92.6%) [rb4] [SK5] described negative implications or barriers to teaching EBPs. We identified themes within these responses if at least three programs noted similar benefits, challenges or barriers. Although respondents could note multiple benefits or barriers related to a theme, a respondent was only counted once per theme.
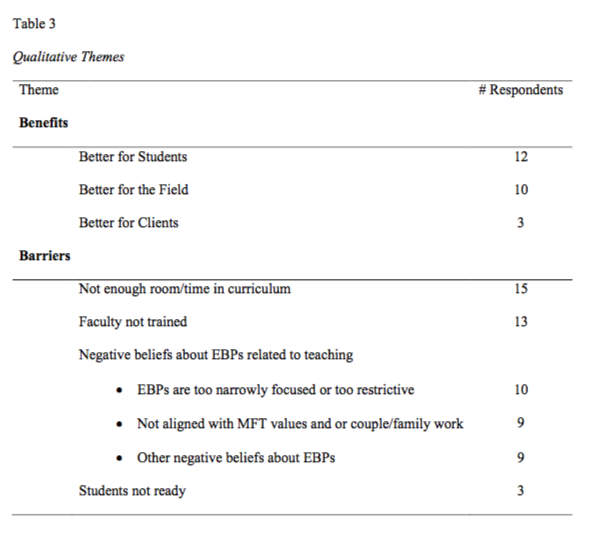
Positive implications. Three themes associated with the positive implications of teaching evidence-based practices were identified (see Table 3): (a) advantages for students; (b) advantages for the profession; and, (c) advantages for clients.
Advantages for students. The most frequently identified benefit (n = 12) was that teaching EBPs was better for students. Advantages noted for students included preparedness and employability. “Better prepared graduates” was described as “literacy about the field,” as well as clinical skill development. Several respondents stated that knowing EBPs creates better clinicians by providing clarity about practice, making it easier to translate concepts and to teach more explicit clinical skills. Respondents indicated this increases students’ confidence, and makes them more marketable. Some stated that employers appreciate the exposure of students to specific EBPs and that graduates were “versed in the use of literature.” One noted that exposure to EBPs in graduate school resulted in quicker promotion to supervisory positions. This relationship between exposure to EBPs and expanded employment opportunities was noted by another respondent as being helpful in recruiting students to their graduate program.
Advantages for the profession. Ten respondents noted that teaching EBPs is better for the discipline of marriage and family therapy. Most noted that marriage and family therapists should be able to demonstrate that their practice is effective, and believed this increases the credibility of the profession. One respondent stated that emphasis on EBPs provides credibility to a field that is “often seen as an art and less of a science.” Another stated that EBPs increase credibility for marriage and family therapy as a “younger” discipline of the behavioral health field. Two respondents noted that it was beneficial to have a strong research base to demonstrate that marriage and family therapy can be more effective than other approaches. Some commented that teaching EBPs helps marriage and family therapists to stay current, “to speak the language of the larger mental health field.” Finally, one respondent highlighted that knowledge of EBPs can help secure research funding and insurance reimbursement.
Advantages for clients. Three respondents identified teaching EBPs as providing an advantage for clients. They stated that learning about EBPs is “good” in order to know what is effective to meet specific client needs. One shared that teaching EBPs leads to students being “more research based and client context-focused.” Another added that “ we want clients to get better and we know there is something that is demonstrated to work that we can use to tweak our treatment and to give us a little help.”
Barriers to teaching EBPs. Six themes (see Table 3) emerged from the 25 programs who responded to the question about perceived challenges or barriers to teaching evidence-based practices. One study participant did not offer a response to that question.[rb8] [SK9] Challenges and barriers were noted by programs that do and do not teach EBPs.
Of the four programs that do not teach EBPs, two identified logistics as the primary barrier (too little room in the curriculum, competing demands and untrained faculty), and did not indicate any negative implications of teaching EBPs for the profession. The remaining two programs noted multiple concerns, with explicit statements about the negative impact EBPs might have on MFT training and practice. For example, “…students become sure and certain, rather than curious and considering. They become skilled workers rather than healers.”
Misconceptions or beliefs were identified by 17 respondents as a challenge or barrier to teaching EBPs. The most frequently cited (n = 10) belief was that EBPs are too narrow in their focus. Responses included that EBPs were not studied with a diverse client population, that they did not take into account the complexity or uniqueness of individuals, or can’t be applied in private practice or small treatment settings. Criticism of EBP research focused upon sample diversity, random controlled trials, and the validity of some findings. Several respondents noted that simply because there is (or is not) research supporting effectiveness of an intervention does not mean a treatment is better (or worse).
Another frequently identified challenge or barrier was lack of room in the curriculum to include content on EBPs (n = 15). These respondents discussed how COAMFTE accreditation standards and licensing requirements determined course content which does not leave time or space for presenting EBPs. Several respondents associated this challenge with having smaller programs and few faculty available to present the required content. Others noted that given this challenge, when EBPs were taught, they could only present overviews of particular models.
Another frequently cited barrier was that faculty are not trained in EBPs (n = 13). This was attributed to the “graying” of faculty who were trained many years ago or who are not currently engaged in clinical practice. Time was a related challenge associated with developing new clinical abilities or to understand newer treatment models. Several respondents noted that senior faculty who are unfamiliar with newer EBP models often present bias and barriers when the program considers teaching EBPs in the curricula. A possible related theme emerged from nine respondents who stated that EBPs are either not aligned with MFT values, or with couples and family therapy, or with the particular theoretical orientation of a graduate program. Some stated a belief that EBPs were more individually focused and not sufficiently focused on couples, families or relational issues or complexities. A few identified misalignment between EBPs and developing clinician engagement skills and competencies. One respondent explained that a main focus of their program is “more on the person of the therapist as the most important ingredient of the therapy relationship, and so transcends any model’s effectiveness.” Another cited their program’s emphasis on social justice and an absence of relevant EBPs with that focus. One respondent did not want to “tell students that they have to practice in a certain way.” Another stated that their program did not teach students manualized approaches, “particularly where there is some entity that is making a profit from the approach.”
Other beliefs about teaching EBPs that respondents identified as barriers (n = 9) included explicit criticism about the design of randomized control trials, cautions about the validity of some findings, and concerns that teaching manualized treatments would limit clinician flexibility.
One additional theme identified by three programs was the perception that students are “not ready” to learn about or use EBPs. This was explained as students not having the ability to understand the research involved with EBPs because as clinicians, they are in a foundational phase just learning to sit with clients. There was concern that some students may not be ready because some “EBPs require you to have a good understanding of your own therapeutic identity,” and some students are not yet at that point in their development.
DISCUSSION
Marriage and family therapy and its seminal practice models, structural and strategic family therapy, emerged with articulation of a systems theory of human communication and behavior (Bateson, 1972) and its application with children, youth and their families (Haley, 1987; Minuchin et al., 1967; Minuchin, 1974; Minuchin & Fishman, 1981). While some early family therapy pioneers like Bowen (1978) attempted to bridge old and new theories, this new theory and these new practice models challenged individually-focused psychodynamic or classic behavioral theories and practices (Nichols & Schwartz, 2006). Those that built upon family systems theory and its logical extension to ecological systems theory (Bronfenbrenner, 1981), as well as upon the lessons from case studies of structural and strategic family therapy, created well-articulated, RCT-tested and disseminated practice models like MST, MDFT and FFT that assess and intervene in systemic behavioral patterns of interaction (Alexander, Waldron, Robbins, & Neeb, 2013; Henggeler et al., 2009; Van der pol, Machteld, Noom, Stams, Doreleijers, van Domburgh, & Vermeiren, 2017). The family systems theory and ecological systems theory supporting the selection of participants, family engagement, assessment and intervention processes of these practice models were tested and adapted with diverse client populations beset by an array of contributing factors to behaviors of concern (Henggeler & Schaeffer, 2010).
In developing curricula, any master’s degree program necessarily must consider the context of organizations and the funding sources where their graduates will be employed. As articulated in Barwick’s (2011) study, administrators and supervisors report that graduates are by-and-large not entering the workforce with the requisite skills to deliver EBP in community-based behavioral health centers. Further, as MFT programs respond to COAMFTE curricula requirements and endeavor to provide training in EBPs, programs do so with a limited number of faculty. While some faculty may be more versed in specific EBPs, others may have philosophical or practical concerns about presenting EBPs to master’s level MFT students.
Most of the responding MFT programs in this study taught elements and activities, theory base and theory of change, and the research supporting an EBP’s application with specific populations. However, concerns about evidence-based practice were similar to those noted in a study of MSW curricula (Bertram, Charnin, Kerns, & Long, 2015) and in development of systems of care. The Child and Family Evidence Based Practice Consortium produced two white papers and a national webinar to address these common concerns and associated misconceptions (Bertram, Kerns, et al., 2015a; Bertram, Kerns, et al., 2015b).
It is wise to ponder what contributes to the persistence of these misconceptions. When we bring our child to a medical doctor we expect and have confidence that the doctor follows tested guidelines for heath or illness assessment and intervention. In behavioral health care, suggested guidelines for assessment and intervention exist in all forms of practice. Because evidence-based practices describe and test these guidelines, they should provide confidence for clients, practitioners, and educators.
LIMITATIONS
The primary limitation of this study is sample size. Although we had a modestly acceptable response rate for survey research (30%), findings would be far more robust with a larger sample size. As in all survey research, respondents were “the willing.” As a result, we could have missed important perspectives from those who did not participate. The survey queried deans and directors of master’s level MFT programs who might not be fully aware of the details of EBP presentation in every course. We attempted to address this limitation by offering the survey questions to MFT program leaders ahead of time so they could engage their faculty in developing the program’s response. Nevertheless, deans and directors do oversee the curriculum and applications for COAMFTE accreditation, so they are aware of faculty discourse and the integration of core constructs across the curriculum. Finally, we had no way to determine if the EBP courses available within the MFT programs were required courses or electives.
IMPLICATIONS
The majority of responding master’s level MFT programs incorporate at least some degree of training in evidence-based interventions with varied depth and breadth of instruction. Our studies suggest that a major source of this variability may be the faculty themselves. In both the MSW study (Bertram, Charnin, et al., 2015) and in this study of masters level MFT programs, respondents highlighted that faculty who did not stay current with development of new practice models, those who do not value research, and those who embrace psychodynamic theory were a barrier to including EBPs in curricula. Integration of EBP within curricula requires thoughtful consideration of how to provide knowledge and opportunities for skill development. Program directors should carefully consider the manner in which curricula changes are made. Instead of faculty discussing whether or not to teach EBPs, it may be helpful to first address common misconceptions, then to discuss how to teach a process of evidence-informed practice, before discussing which specific evidence-based practice models should be taught.
REFERENCES
Ackerman, N. W. (1961). A dynamic frame for the clinical approach to family conflict. In N. W. Ackerman, F. L. Beatman, & S. N. Sherman (Eds.), Exploring the base for family therapy (pp. 52–67). New York, NY: Family Service Association of America.
Alexander, J.F., Waldron, H.B., & Robbins, M.S., & Neeb, A.F. (2013). Functional Family Therapy for Adolescent Behavior Problems. Washington, DC: American Psychological Association.
American Association for Marriage and Family Therapists. (2004) Marriage and family therapy core competencies. Retrieved from http://www.aamft.org.
American Psychological Association Presidential Task Force on Evidence Based-Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61(4), 271-285. doi:10.1037/0003-066X.61.4.271
Barwick, M. (2011). Master’s level clinician competencies in child and youth behavioral healthcare. Emotional & Behavioral Disorders in Youth. 11(2), 32-29.
Bateson, G. (1972). Steps to an ecology of mind. New York, NY: Ballantine.
Baucom, D.H., Shoham. V., Muescr, K.T., Daiuto, A.D., & Stickle, T.R. (1998). Empirically supported couple and family interventions for marital distress and adult mental health problems. Journal of Consulting and Clinical Psychology, 66, 53-58.
Bertram R.M., Blase, K.A., & Fixsen, D.L. (2015). Improving programs and outcomes: Implementation frameworks and organization change. Research on Social Work Practice, 25(4), 477-487.
Bertram, R.M., Charnin, L.A., Kerns, S.E.U., & Long, A.C. (2015). Evidence-based practices in North American MSW curricula. Research on Social Work Practice, 25(6), 737-748.
Bertram, R.M., Kerns, S.E.U., Bernstein, D., Mettrick, J. Marsenich, L., Kanary, P., & Choi, S.W. (2015). Evidence-informed practice in systems of care: Misconceptions and facts; and Evidence-informed practice in systems of care: Frameworks and funding for effective services. Technical Assistance Network for Children’s Mental Health Network, US Department of Health and Human Services Substance Abuse and Mental Health Services Administration, Washington D.C.
Bowen, M. (1959). Family relationships in schizophrenia. In A. Auerback (Ed.), Schizophrenia: An integrated approach (pp. 147–178). New York, NY: Ronald.
Bowen, M. (1978). Family therapy in clinical practice. Northvale, NJ: Aronson.
Bronfenbrenner, U. (1977). The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press.
Bruns, E.J., Kerns, S.E.U., Pullmann, M.D., Hensley, S.W., Lutterman, T., & Hoagwood, K.E. (2015). Research, data, and evidence-based treatment use in state behavioral health systems, 2001–2012. Psychiatric Services, 67(5), 496-503.
Chambless D.L., & Hollon S.D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology, 66, 7–18.
Chambless, D.L., & Ollendick, T.H. (2001). Empirically supported psychological interventions: Controversies and evidence. Annual Review of Psychology, 52, 685-716.
Commission on Accreditation for Marriage and Family Therapy Education. (2017). Accreditation standards: Graduate & post-graduate marriage and family therapy training programs, version 12.0. Alexandria: VA: Author.
Council on Social Work Education. (2015). Educational policy and accreditation standards. Alexandria, VA: Author.
Crane, D.R., Wampler, K.S., Sprenkle, D.H., Sandberg, J.G., & Hovestadt, A.J. (2002). The scientist-practitioner model in marriage and family therapy doctoral programs. Journal of Marital and Family Therapy, 28, 75-83.
Drabick, D.A., & Goldfried, M.R. (2000). Training the scientist– practitioner for the 21st century: Putting the bloom back on the rose. Journal of Clinical Psychology, 56, 327–340.
Duncan, B.L. & Miller, S.D. (2000). Clients theory of change: consulting the client in the integrative process. Journal of Psychotherapy Integration, 10(2), 169-187.
Fixsen, D.L., Blase, N.S., Naoom, S.F., & Wallace, F. (2009). Core implementation components. Research on Social Work Practice, 19(6), 531-540.
Frank, G. (1984). The Boulder Model: History, rationale, and critique. Professional Psychology: Research and Practice, 15, 417-435.
Haley, J. (1987). Problem-solving therapy (2nd ed.). San Francisco, CA: Jossey-Bass.
Henggeler, S.W., & Schaeffer, C.M. (2010). Treating serious emotional and behavioural problems using multisystemic therapy. Australian and New Zealand Journal of Family Therapy, 31(2), 149-164.
Henggeler, S.W., Schoenwald, S.K., Borduin, C.M., Rowland, M.D., & Cunningham, P.B. (2009). Multisystemic therapy for antisocial behavior in children and adolescents (2nd ed.). New York, NY: Guilford Press.
Institute of Medicine. (2001). Crossing the quality chasm: A new healthy system for the 21st Century. Washington, DC: National Academic Press.
Karam, E.A., & Sprenkle, D.H. (2010). The research-informed clinician: A guide to training the next generation MFT. Journal of Marital and Family Therapy, 36(3), 307-319.
Kaslow, F. (2007). A brief history of the field of family psychology and therapy. Handbook of EMDR and Family Therapy Processes, 438-454.
Kazdin A.E., Bass D., Ayers W.A., & Rodgers A. (1990). Empirical and clinical focus of child and adolescent psychotherapy research. Journal of Consulting and Clinical Psychology, 58(6), 729–740.
Meyer, A.S., Templeton, G.B., Stinson, M.A., & Codone, S. (2016). Teaching research methods to MFT master’s students: A comparison between scientist-practitioner and research-informed approaches. Contemporary Family Therapy: An International Journal, 38(3), 295-306.
Minuchin, S., Montalvo, B., Guerney, B.G., Rosman, B. L., & Schumer, F. (1967). Families of the slums: An exploration of their structure and treatment. New York, NY: Basic Books.
Minuchin, S. (1974). Families and family therapy. Cambridge, MA: Harvard University Press.
Minuchin, S., & Fishman, H.C. (1981). Family therapy techniques. Cambridge, MA: Harvard University Press.
Nichols, M.P., & Schwartz, R.C. (2006). Family therapy: concepts and methods (7th ed.). Boston, MA: Allyn & Bacon.
Oka, M., & Whiting, J. (2013). Bridging the clinician/researcher gap with systemic research: The case for process research, dyadic, and sequential analysis. Journal of Marital and Family Therapy, 39(1), 17-27.
Owenz, M., & Hall, S.R. (2011). Bridging the research–practice gap in psychotherapy training: Qualitative analysis of master’s students’ experiences in a student-led research and practice team. North American Journal of Psychology, 13, 21–34.
Parker E.O., Chang J. & Thomas V. (2016). A content analysis of quantitative research in journal of marital and family therapy: A 10-year review. Journal of Marital and Family Therapy, 42(1), 3–18.
Patterson, J.E., Miller, R.B., Carnes, S., & Wilson, S. (2004). Evidence-based practice for marriage and family therapists. Journal of Marital and Family Therapy, 30(2), 183-95.
Pinsof, W., & Wynne, L. (Eds.). (1995). Special issue: The effectiveness of marital and family therapy. Journal of Marital and Family Therapy, 21(4).
Raimy, V (Ed.). (1950). Training in clinical psychology. New York, NY: Prentice Hall.
Satir, V. (1964). Conjoint family therapy. Palo Alto, CA: Science & Behavior Books.
Sexton, T.L., Alexander, J.F., & Mease, A.L. (2004). Levels of evidence for the models and mechanism of therapeutic change in family and couple therapy. In M. J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (5th ed., pp. 590-646). New York, NY: Wiley.
Shadish, W. J., Ragsdale, K., & Glaser, R.R. (1995). The efficacy of marital and family therapy: A perspective from meta-analysis. Journal of Marital and Family Therapy, 21, 345-360.
Silverman, W.K., & Hinshaw, S.P. (2008). The second special issue on evidence-based psychosocial treatments for children and adolescents: A 10-year update. Journal of Clinical Child and Adolescent Psychology, 37, 1–7.
Sprenkle, D.H. (2003). Effectiveness research in marriage and family therapy: Introduction. Journal of Marital and Family Therapy, 29(1), 85-96.
Stith, S.M. (2014). What does this mean for graduate education in marriage and family therapy? commentary on “The divide between ‘evidenced–based’ approaches and practitioners of traditional theories of family therapy.” Journal of Marital and Family Therapy, 40(1), 17-19.
Van der pol, T.M., Machteld, H., Noom, M.J., Stams, G.J.M., Doreleijers, T.A.H., van Domburgh, L., & Vermeiren, R.R.J.M. (2017). Research review: The effectiveness of multidimensional family therapy in treating adolescents with multiple behavior problems – a meta-analysis. Journal of Child Psychology and Psychiatry, 58(5), 532-545.
